New publication
Personalised, GIS-based counselling to promote habitual walking
BMC Geriatrics (2025) 25:471
Timo Hinrichs, René Schilling, Alexandros Sofios, Denis Infanger, Luisa Prechtl, Nora Stauffer, Viviane Eichenberger, Eleftheria Giannouli, Taina Rantanen, Erja Portegijs, Corina Schuster-Amft, Anna Mai, Arno Schmidt-Trucksäss, Christina Röcke & Robert Weibel
Background
Physical activity is a cornerstone of health for older adults. Recent evidence underscores that even regular light activity, such as routine walking, offers substantial health benefits. Traditional approaches to promoting walking often overlook the importance of the local neighbourhood environment and the wide range of abilities and preferences of older adults. A personalised walking intervention – emphasizing personal preferences and local facilitators by employing Geographic information System (GIS)-based methods for communication and goal setting – might help to overcome problems of low long-term adherence to walking interventions.
The MOBITEC-Routes trial aims to assess the effects of personalised, GIS-based walking promotion – versus general information on determinants of health – for mobility-limited and chronically ill older adults on walking (primary outcome) immediately after the 15-week intervention period (primary endpoint) and after another 8 months of follow-up (secondary endpoint).
Methods
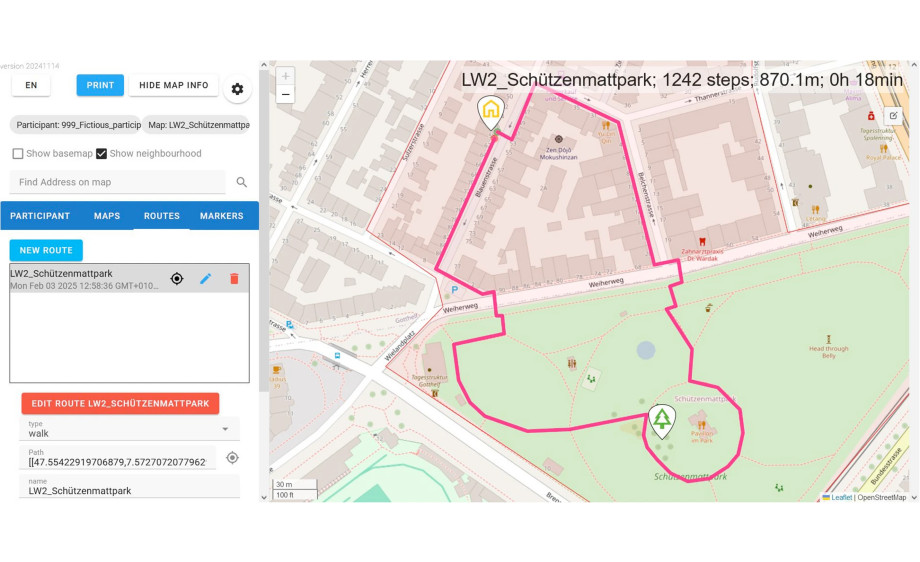
This prospective, two-arm, single centre randomised controlled trial targets sedentary, mobility-limited, chronically ill, and community-living older adults aged 65 + (target N = 130). Outcomes are assessed after 15 weeks of intervention and after an additional 8 months of follow-up. The experimental intervention offers personalised promotion of habitual walking, delivered by an exercise professional in face-to-face and telephone sessions. Opportunities to increase leisure as well as utilitarian walking are identified by using interactive digital maps, personalised walking routes are co-created by the exercise professional and the participant, and a personalised activity plan is developed. Behaviour change strategies are employed. The control group receives general information on determinants of health. Outcomes include walking (average steps per day; primary outcome), time spent lying, sitting, standing and stepping, physical function, life-space mobility, health-related quality of life, fall-related self-efficacy, active aging, as well as constructs of the Health Action Process Approach (HAPA) model (secondary outcomes). Effects will be analysed by analysis of covariance (ANCOVA; primary analysis intention-to-treat, complemented by per-protocol).
Discussion
By incorporating personal preferences and the neighbourhood environment, this intervention aims to promote walking as a sustainable and meaningful part of everyday life for mobility-limited and chronically ill older adults. If the personalised GIS-based approach is successful, it could be seamlessly integrated into preventive healthcare strategies.
https://doi.org/10.1186/s12877-025-06113-2